



 8 comments have been left for this article.
8 comments have been left for this article. BP Comment Quick Links

|

|
December 9, 2011 Collateral DamageRounding Up the Usual Suspects: The Torn ACL
Running down the first base line, the last thing Jason Castro expected in a spring training game was that in less than a second his season would be over. It’s something he had done a hundred times before without any inkling of an injury, and yet this time, for whatever reason, he ended up paying for it. As he tried to avoid the tag by Miguel Cabrera, his knee twisted awkwardly, and before he knew it he was done. Castro tore the anterior cruciate ligament (ACL) in his knee along with his meniscus and underwent surgery early in March 2011. Injuries to the ACL, while more common in soccer, basketball, and football, still occur in baseball across all ages and experience levels. The ACL is usually torn in a non-contact, decelerating, twisting injury that stretches the ACL until its point of failure. ACL injuries are not new; in fact, the first surgery to reconstruct the ACL intraarticularly—inside the joint—was done back in 1917. Yes, almost 100 years ago. It used to be that ACL injuries were career-ending or career-altering, but as more research and better equipment was developed, the surgery became more commonplace, and the recovery time was reduced. Now, there are about 100,000 ACL surgeries each year, and over 200,000 ACL injuries. It seems that almost everyone has known someone or known of someone who has suffered an injury to the ACL. Anatomy
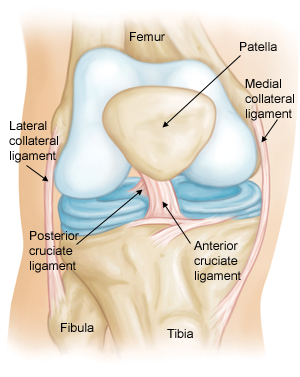
Figure 1: Normal knee anatomy The knee is a hinged joint, and the ACL is one of its four main ligaments. The ACL is vital to the long-term health of the knee. Measuring only about three to four centimeters long and one centimeter wide, it originates from the back edge of the lateral femoral condyle and inserts toward the front aspect of the tibia, slightly off-center. It’s actually made up of two bundles that overlap each other like your fingers do when crossed. Biomechanics/Function
Figure 2: Two bundles of ACL http://www.performanceorthosports.com/WEBPAGES/db_acl_1_wrmc_newlsetter_jpeg.JPG The two bundles are the key to the ACL’s stabilizing function, which is to limit forward translation of the tibia and provide rotational stability to the knee. The smaller anteromedial bundle is tight in flexion, while the larger posterolateral bundle is tight in extension. Having the different bundles present helps to stabilize the knee throughout its functional range of motion. Hyperextension and internal rotation, such as planting the foot and cutting to the opposite direction, places the ACL at its greatest risk of injury. The majority of injuries to the ACL are non-contact in nature, such as directional changes or awkward landings from a jump, with only about one-third being the result of direct contact like a collision in football. Interestingly, females are more prone to ACL injuries for reasons ranging from lower extremity alignment differences to the effects of estrogen on the ligaments. Despite the widespread belief that it’s easy to tear the ACL, there are much easier parts to injure. The average force needed to rupture the ACL is about 500 pounds applied directly. This may not seem like a lot, but the total force dissipated by the knee is usually significantly greater.
Symptoms/Findings In the doctor’s office, the clinician will put the knee through a variety of tests to evaluate how loose the ligament feels. Then, an MRI will usually be ordered to confirm the clinical diagnosis, of which we have an example below.
Figure 3: Normal ACL
Figure 4: MRI image of torn ACL In the first image above of a normal ACL, you can see a distinct dark line running from the back of the femur to the front part of the tibia. There is no white signal signifying swelling in the ligament that would indicate a partial tear, and it looks to be well-organized, with the fibers all running in the same direction. In figure 4, you can see that there is no distinctness where the ACL was, and the fibers are running in different directions. Partial tears have some resemblance to a normal ACL, but there may be swelling in the ligament or the ligament may be noticeably thicker in one area.
Treatment
Surgical options Small portions of all of these autologous tissues are used to at least double the tensile strength of the original ACL. During ACL reconstructions using a bone-patellar-bone autograft, two standard arthroscopic portals are used in addition to a central incision. A five-to-seven centimeter incision is made over the patellar tendon to allow the harvesting of the graft. Roughly one-third of the patellar tendon is removed—don’t worry, we have enough to spare—along with a small portion of bone that is attached to each end. The graft is then removed from the knee and prepared for the reconstruction. While the graft is being prepared, attention is turned to the other structures in the knee. The surgeon ensures that there will be enough room between the bones for the new ACL by smoothing down or burring away any excess material. The surgeon then lines up the tunnels through the femoral condyle and tibia for the new ACL. Once the first portion of the graft is passed through, it’s secured to the femur. The knee is then bent to 30 degrees to put the proper amount of tension on the new ACL before it is secured to the tibia.
Figure 5: ACL graft tunnels The surgeon then moves the knee around while looking in the arthroscope to make sure the graft is not getting pinched between the bones and has the proper tension. After the area is irrigated, the wounds are closed and the patient is placed into a post-operative brace. Using the hamstring tendons as a graft choice entails a different procedure. This is usually all done arthroscopically, which makes it more comfortable post-operatively but does not change long-term plans. This approach has a minimally higher re-injury rate, but re-injury rates are fairly dependent on the skill of the surgeons. In order to harvest the hamstring tendons, the knee is placed into a figure-4 position. An incision is made a small distance from the middle of the tibia. After dissecting down, a tendon stripper—yes, that’s what it’s called—is used to remove a portion of the distal hamstring tendons. The tendon graft is then prepared before being guided through the tunnels as described above.
Post-Operative Treatment
Youth ACL injuries However, there is a surgical technique that can reconstruct the ACL without injuring the growth plates. It involves taking a portion of the ITB tendon on the lateral side of the knee, splitting it, and winding it both inside and outside of the knee joint before being attached. It has been shown to be very effective and allows the athlete to return to his or her desired sport without restrictions (except for wearing a brace).
Summary
Corey Dawkins is an author of Baseball Prospectus. Follow @CoreyDawkinsBP
|
Does a torn ACL tend to have any long-term consequences - reduced speed or agility, or greater difficulty in catching, or is it something that, once healed, is not an issue?
Isolated ACL injuries without meniscus or cartilage tears come back really without any issues once fully rehabilitated. Sometimes full recovery including agilities can take up to a year or so. Some people do have a small decrease in speed or motion but that is usually the result of excess scar tissue buildup.